
TRAUMA-RESPONSIVE ORGANIZATIONAL APPROACHES TO GRIEF PROCESSING AND HEALING: COVID-19 AND BEYOND

The necessary and profound public health response to the COVID-19 pandemic has highlighted the reality that there is no ‘right time’ to do what needs to be done. Lives have been saved by the mandatory changes in lifestyles and daily routine. And still, it is painful. To safeguard our health and that of essential workers, some people, more than others, can stay at home and limit their community outings. In many ways, we have chosen to adapt. In other ways we struggle. There have been various and significant losses. Life as we knew it has been disrupted. While still in the thick of it, we have yet to fully understand and count all the costs.
This informal guidance document will provide suggestions about trauma-responsive organizational approaches to grief and healing. Many organizations, whether public or private, volunteer-driven or employee-based, small or large, and regardless of their sector, have expressed concern about helping their staff and stakeholders cope with and heal from COVID-19.
In keeping with Alive and Well Communities’ focus on changing the culture, practices and structure of systems that affect communities, we are offering suggestions to organizational leaders, service providers, and decision makers (of which there are many). Though we believe there should be guidance about promising practices for direct care delivery, this is not a document about clinical approaches to counseling. Most of the people we encounter in organizations are not counselors. Further, we know that one does not have to be a therapist to be therapeutic. With each relationship and in each interaction, there exists both the potential to perpetuate harm and the opportunity to support healing. Alive and Well Communities honors and call us all to recognize the unique grief processing and healing needs related to racial identities, ethnicity, immigration status, religious practices, gender identity, and sexual orientation. This guidance focuses on helping our partners and other organizations think about and plan for how they can facilitate healing as we apply the ‘trauma lens.’ We use the trauma lens when we seek to understand and explain people’s verbal expressions and behaviors by first asking ourselves “what happened to” a person rather than questioning “what is wrong with” a person. We focus on healing because the goal of trauma-informed care and equity is to promote restored wellness and/or wholeness of being. Providing supports for healing enables improved resilience, satisfaction, healthier relationships, and optimal life performance.
This informal guidance is grounded in four core beliefs:
In order to heal, we must acknowledge grief and give space to process the causes. Grief is commonly defined as an individual or collective response to loss or change. we typically think of grief in terms of death; yet, grief can arise from changes in job responsibilities, loss of financial stability, loss opportunity, impaired relationships, and so much more. Instead of deeply engaging with the pain of loss and change, we may sometimes feel pressure to ‘move on’ and quickly ‘bounce back.’ as such, we may not thoroughly process the hurtful experience and instead mask our grief with activity and unhealthy coping strategies. The speed of our systems places priority on being efficient at the expense of being well.
Though the full impact is unknown, COVID-19 is a sudden and complete disruption to life as we know it. There is inherent ‘loss’ to that disruption. In many ways our communities, nation, and world have experienced collective trauma. Trauma is defined as an event or series of events that overwhelm a person or community’s ability to cope in a healthy manner while carrying out life’s roles, responsibilities, relationships, and interactions.
There is no “typical” grief trajectory. The impact of each loss or change is unique to each person and/or community. Loss and change can activate hot and cold emotions (e.g. rage and/or detachment).
In essence, organizations are a collection of people who formally come together to meet needs by providing a specific product or delivering specific services. As a collective, the losses experienced among an organizations’s people are within its duty to own and power to help heal.
In many ways, people and institutions are mutually dependent. People depend on organizations for financial stability, discretionary goods/services, essential resources, health and human services, among other needs. An organization is shaped by the experiences of the people within and around it. The health, well being, and level of resources of an organization’s stakeholders affect the institution. In customer-facing interactions and during internal processes, an organization ‘experiences’ the awareness, successes, and sufferings of its people. We do not intend to suggest that grief within an organization’s circle of concern is simply a sum of individual sorrows. Instead, we are proposing that community trauma and collective overwhelm require individual, community-level, and organization-level healing.
We know that during crises in general and throughout the reopening of our society during COVID-19, there will be a combination of grief and relief. The natural reactions that follow surviving such a significant community event will need to be recognized and thoughtfully managed. Carefully considered approaches are needed to address the immediate effects of people’s overwhelm and the lingering effects of loss and change.
TRAUMA AND THE GRIEF PROCESS: WHAT TO EXPECT
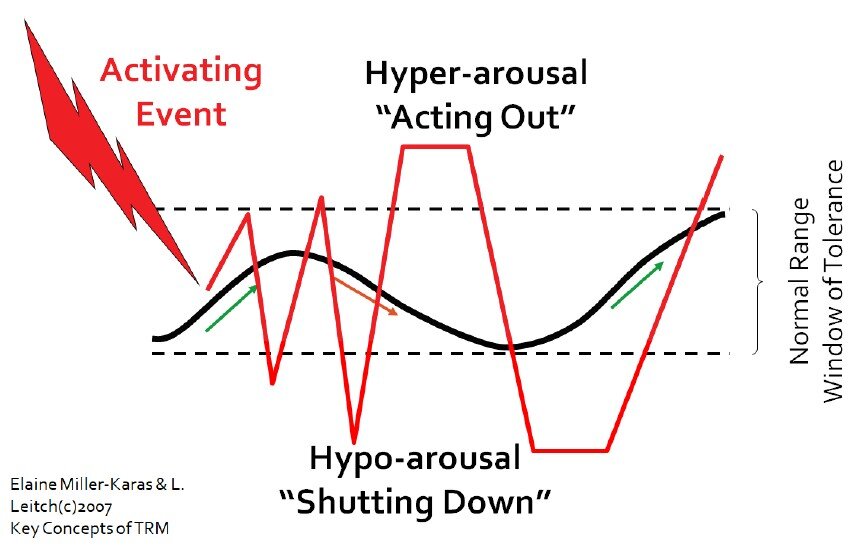
There is no standard way to grieve the losses and change people experience. Grief takes many forms and lasts through different time frames. Some loss or change overwhelms a person’s ability to cope (i.e. is traumatic). Grief and trauma are not synonymous, but they can coexist. Trauma science shows us that grief processing can influence how much additional stress a person can tolerate in the moment and how they show up during interactions with others. Being overly burdened narrows a person’s window of stress tolerance. The window of stress tolerance marks the cumulative limits of how much more a person can bear, in each moment, before they automatically begin to act out, freeze, or shut down. The potential for overwhelm is not an indicator of strength, character, interest, or will.
It is a matter of how much additional threat to psychological or physical safety a person can tolerate, given what they have already experienced. The thresholds for becoming overwhelmed are as unique as each individual’s experience of grief, stress, and healing. People can cycle through periods of healthy calm, acting out, freezing, and/or shutting down as they experience the effects of stress and reminders of what has been lost/changed. Becoming trauma-responsive requires individuals and organizations to implement practices that normalize an empathetic and healing-centered approach to those acting out, freezing, or shutting down stress-responses.
Reactions to loss can be physical and psychological. It is common for a grief process to include:
Longing, crying, thinking of who/what was lost, anger, denial, sadness, despair, insomnia, fatigue, guilt, loss of interest, confusion, body pains, disorganization, disbelief, inability to concentrate, preoccupation with thoughts, loss of appetite, over-reacting, numbness, relief, sadness, yearning, fear, hair, nail, and skin concerns, shame, loneliness, helplessness, hopelessness, emptiness, etc...
While each grief process is unique, a “typical” grief process eventually moves towards connection and healing. Cultural norms and expectations around grief serve to guide us in this direction. The current public health crisis due to COVID-19 is disrupting these norms and compounding stress during an already difficult time. While “physical distancing” is critical in order to prevent the spread of COVID- 19, it is incredibly important to consider how the removal of social gatherings to engage in the ‘expected’ grief process will impact individuals, organizations, and communities. In addition to grief, bereavement and mourning are critical parts of how people process loss. Bereavement is the state of having experienced the loss of someone or something with whom there is a close relationship. Mourning is the range of cultural norms and traditions associated with death. The norms help those experiencing loss find meaning and begin to imagine a new reality.

A typical or expected grief process is marked by movement towards acceptance of the loss and a gradual alleviation of the symptoms – the ability to engage in basic daily activities and move towards meaning making. When an individual and/or community starts moving towards isolation, blame, and disconnection, the grief process is at risk of becoming more harmful and long-lasting. These too are normal potential responses that can be addressed with adequate and responsive support for healing. To facilitate healing-centered approaches to grief and stress, the guidance in this document is informed by the principles of trauma-informed care: trustworthiness, equity, choice, collaboration, empowerment, and safety.
TRAUMA-RESPONSIVE ORGANIZATIONAL APPROACHES TO GRIEF PROCESSING AND HEALING
In keeping with the four stages of The Missouri Model: A Developmental Framework for Trauma Informed Approaches, this informal guidance about organizational responses to grief and healing aligns with the continuum of trauma-informed organizational change. The strategies presented here are not exhaustive. This guidance focuses on organizational leaders’ and service providers’ awareness and practical strategies to more sensitively respond to the internal and external needs that arise from loss and change. The four stages of the Missouri Model are: Trauma Aware, Trauma Sensitive, Trauma Responsive, and Trauma Informed. Below each stage are several suggestions that organizational leaders, service providers, and decision makers might consider to support the healing of stakeholders.

1 Trauma Aware
At this stage, organizational leaders and service providers understand the prevalence and signs/symptoms of trauma for employees, the organization, and those it serves.
Organizational leaders and service providers seek to understand which types of losses and to what extent employees, clients, and those in the broader community are affected by life disruptions and losses related to the current crisis
Leaders and providers seek to reconcile current losses with existing accumulations of stress and deprivation which may compound social, emotional, physical, psychological, and work-related challenges.
Examples:
In education, a school district maintains its momentum around implementing trauma-informed care by offering trauma-related training. The district continues to reflect on and refine its trauma-informed care implementation plan.
In healthcare, practitioners and organizations seek to understand how individuals’ identities, personal and community history, and social determinants of health are affecting illness, death, and disease that may cause loss and grief, during COVID-19, before, and beyond.
Government entities may demonstrate trauma awareness by seeking to understand and acknowledge the role political power has in losses related to the current moment. Decision makers actively seek to analyze if and how historical narratives promote healing and well being. They seek to understand if and to whom there is inequitable distribution of loss, disruption, disease, and death.
2 Trauma Sensitive
At this stage, organizational leaders and service providers actively seek to understand the nuanced ways trauma affects its employees, the organization, and those it serves. Decision makers adjust policies and practices after applying nuanced knowledge of its resources and information about the crisis- and trauma-related needs of its stakeholders.
Leaders and providers seek to understand which needs of its circle of concern have been affected in general, and specifically as relates to the organization’s services, specializations, and corporate social responsibility (CSR) initiatives.
Leaders regularly connect with internal stakeholders and those it serves to act on its values around care and concern. Service providers develop a routine approach to regularly contacting and assessing the needs, resource gaps, and impact of the current crisis on those they serve.
Leaders create intentional space and time for staff and stakeholder connections. They work collaboratively to establish rituals for mourning and healing, including for themselves.
Examples:
Organizational leaders across sectors setup feedback opportunities to document and track the resource needs and impact the current moment has on its clients, employees, and partners.
Customer service personnel across industries have been trained on how to respond to dissatisfied customers, in general, or those with specific needs related to loss. Customer service personnel are trained and coached to respond to customer’s verbal and behavioral dysregulation with empathy and an understanding that conflicts may be related to stress, loss, and grief processing.
Government entities question what is needed to support healing and repair. By collaborating with affected community members, decision makers seek to clarify the complex relationships between disparate impact of policies, loss, and grief.
3 Trauma Responsive
At this stage, organizational leaders and service providers identify efficient and powerful levers to support grief processing and healing. Decision makers initiate policy and practice change after evaluation of current processes, reconciling stakeholder needs, and planning targeted actions.
Organizational leaders and service providers maintain high standards while providing targeted supports that help stakeholders manage their unique grief process, meet trauma-sensitive performance expectations and supervision processes.
Leaders and staff evaluate performance management and human resource processes through the lens of trauma to determine which policies support processing through the grief or penalize potential stress responses associated with overwhelm (e.g. acting out, freezing, and/or shutting down).
Leaders adjust leave policies, bereavement policies, virtual office arrangements, thresholds for what qualifies as a “significant life event,” and the employee assistance program to ensure needed resources and services are provided at low to no cost for employees and in a timely manner.
Leaders and staff establish referral relationships and service agreements with providers of individual, family, in-person, and virtual grief counseling for those they serve.
Examples:
The education sector’s trauma-responsive approach to grief and COVID-19 may involve boards of education and educational administrators developing a strategic plan for how to structure the beginning of the semester to add closure to the abruptly ended school year. Decision makers collaborate with school staff to plan activities with adults/parents/students to enable a culture of healing and set shared expectations about workload and work pacing. Leaders prioritize high expectations and meeting adult and youth’s social and emotional needs related to the loss and changes of transitioning to/from online and in-person education.
Government entities implement immediate- and long-term policies and regulations to repair harm and losses from the disparate impact of policy for the current moment and beyond. The goal of restoration is codified in measurable metrics and supporting actions. Decision makers establish processes for tracking outcomes to ensure the most aggrieved are receiving the most direct and healing-centered actions.
4 Trauma Informed
At this stage, organizational leaders and service providers continually adapt policies and practices to support grief processing and healing from trauma.
Organizational leaders and service providers continuously monitor historical and current circumstances that contribute to collective and/or community grief and trauma.
Decision makers update policies, practices, and procedures in a timely fashion to reflect current circumstances and needs. Decision makers and service line leaders routinely adjust formal policies across service lines. Leaders ensure alignment throughout the organization’s structure and hierarchy, as the times and context require. They ensure flexibility in various organizational programs to meet the diverse grief- and healing-related needs of current employees.
Leaders and affected stakeholders regularly collaborate to refine healing-centered metrics and co-construct actions that support grief processing, healing, and restoration.
Examples:
In education, leaders of colleges, schools, and school districts establish processes for routinely supporting their peer organizations. Leaders engage in inter-organizational collaboration to bridge gaps for less resourced community institutions. To strengthen the community’s response to grief, decision makers create opportunities for peer connection and establish processes for sharing organizational knowledge and resources that support healing.
Government entities drive and monitor progress on the restorative metrics, ensure real-time outcomes are tracked, and regularly dialogue about impact with the affected communities. To prevent loss and attend to restoration, course corrections are implemented with urgency and precision.
Grief, bereavement, stress, and trauma have been an ongoing element of individual life, community dynamics, and organizational reality. The public health response to COVID-19 adds the element of losing multiple streams of connectedness when we need it most. We’ve lost connection as we are required to maintain physical distance and adjust how we engage our social networks, if we can engage them at all. From this shared experience of social isolation and economic shutdown, we have learned that grief can take many forms including grieving the loss of life patterns, adjustment of wages, jobs changes or unemployment, housing instability, and loss of residence. There is also the sorrow from losing a loved one and, in context of COVID-19, the lack of closure due to restrictions on traditional ways of commemorating the passing of family members, colleagues, and friends, not to mention the many losses we cannot identify.
We have all lost so much; some more than others. The trauma-responsive approaches presented here are meant to inspire assessment of current resources, clarification of needs, and identification of gaps related to organizational supports for grief processing and healing. Understanding grief, in general, helps us understand what we are seeing after people experience loss/change, helps us remember to apply the trauma lens to verbal expressions and behaviors in the moment, and supports our ability to be more sensitive to people’s lingering reactions to loss and suffering. As organizations consider how to implement structures and practices to support healing, we cannot overemphasize the importance of needs assessment and real-time collaboration with those in the organization’s circle of concern.
We invite organizational leaders, service providers, and decision makers to consider the following reflection questions as they evaluate current structures that support grief processing and determine how to more responsively support healing among the organization’s people and within the organization itself. These questions are applicable to COVID-19 and beyond.
During this time of COVID-19, what have you lost, personally and professionally? What have we lost? Consider loss of life and loss of experiences, loss of normal, loss of future, etc.
How have your community and diverse organizational stakeholders been individually socialized to process grief and healing? How has that been shaped by their identities/culture? How have those norms been disrupted?
How has your organization responded to loss and grief historically? What has your organization done well? Through which processes and in what ways can the organization continue to evolve its response to loss, grief, and healing?
Alive and Well Communities activates communities to heal.
We do this together by:
Elevating community wisdom centering those who have experienced trauma as leaders of the work.
Disrupting systemic oppression and responding to the impact of historical trauma.
Acting with urgency, not waiting for another day or generation.
Leading innovative solutions based on the science of trauma, toxic stress and resiliency.